The Pain of Painlessness: Congenital Insensitivity to Pain with Anhidrosis - A Case Review


Written by Teah Mackay
Neurophysiology Scientist - Alfred Hospital
In the vast expanse of neurological mysteries, one enigmatic paradox has captured attention—the haunting phenomenon known as Congenital Insensitivity to Pain with Anhidrosis (CIPA).
My name is Teah Mackay, and I am fortunate to be a neurophysiologist employed at Alfred Hospital. I have also been lucky enough to have developed clinical experience working at Australia's largest paediatric hospital, The Royal Children's Hospital, and Queensland's largest neurology service, Corbett and Coastal Neurophysiology Services. Through this work I have witnessed the silent struggles of those ensnared by rare neurological disorders.
Arguably one of the most haunting neurology paradoxes is CIPA, a condition where those affected cannot experience pain or produce sweat. Though incredibly rare, this disease captured my attention due to its ironic widespread painful impact on those affected and the challenges it poses to individuals, care givers, families and medical professionals in terms of both early intervention and long term management.
Through Neurophysiology Sciences Society of Australasia communication opportunities, I hope to raise awareness within the neurophysiology community about CIPA, bringing attention to this rare and consequently overlooked disorder and highlighting the challenges faced by those with lived experience.
Congenital insensitivity to pain with anhidrosis case review:
CIPA, also known as hereditary sensory autonomic neuropathies type IV, is an extremely rare autosomal recessive disorder characterised by the inability to perceive pain and regulate body temperature through sweating. CIPA is caused by biallelic mutations in the neurotrophic tyrosine receptor kinase 1 gene (NTRK1), which encodes tropomyosin-related kinase A (TrkA), a receptor for nerve growth factor (NGF) [1].
The absence of NGF-dependent primary afferent neurons with unmyelinated C-fibers and sympathetic postganglionic neurons, in individuals with CIPA leads to the lack of pain sensation and anhidrosis, respectively [2]. Mitochondrial abnormalities in muscle cells and a lack of innervation of eccrine glands are also observed in individuals with CIPA [2].
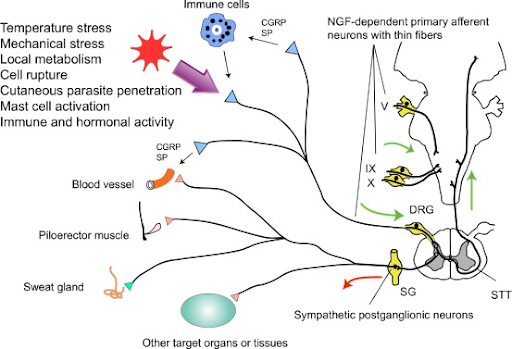
Fig 1. The neurological pathway demonstrates the typical response and interactions of the NGF-dependent primary afferents and sympathetic postganglionic neurons [3].
These physiological abnormalities result in a range of clinical manifestations, including mild to severe developmental delay, recurrent hyperthermia, insensitivity to pain, and self-mutilating behaviour [3]. The incidence of CIPA is estimated to be about 1 in 125 million, although some reports suggest a higher prevalence in specific populations, such as the Negev Arabs and the Vittangi village in Sweden [5]. Patients often experience joint injuries, fractures, and self-mutilation due to the lack of pain sensation. Consequently, approximately 20% of individuals with CIPA die from hyperthermia by the age of 3 [6].
Clinically, patients with CIPA typically exhibit two types of responses to painful stimuli: Insensitivity to pain where the painful stimulus is not perceived at all, and/or indifference to pain where the stimulus is perceived but elicits no response [7]. Patients with different phenotypes of CIPA may experience profound developmental delay [8]. The spectrum of developmental delay in patients with CIPA is determined by which Ntrk1 protein domain a mutation has occurred [8].
CIPA can present with various clinical and subclinical features, examples of these manifestations has been documented in numerous case studies.
Case Study 1: A boy with Autism Spectrum Disorder who experienced CIPA: A case report [9]
A boy developed a high fever at 3 months of age. He suffered from recurrent episodes of uncontrolled fever due to unknown causes, and antipyretics were ineffective. In addition, the child had no painful reaction to any injection. When his first teeth appeared, he began to bite his tongue, fingernails, and toenails repeatedly without any feeling of pain. Subsequently, other members of his family noticed that he was incapable of experiencing pain, and the self-mutilation continued until 48 months. When the boy started walking independently, he was more likely to fall in comparison to his peers. He did not however suffer from any bone fracture or dislocation. The patient could talk at 24 months but could not speak complete sentences until 48 months. Notably, he often did not respond when people called him. Hyperactivity and inattentiveness were also observed [9].
Case Study 2: A case report of CIPA [10]
A 2.5-year-old boy with clinical features of CIPA presented as the first documented cases of CIPA in Iran. The symptoms included recurrent episodes of hyperthermia and unexplained fever that began in early infancy, anhidrosis, profound loss of pain sensitivity, neurodevelopmental delay, unconscious self-mutilation of fingers, lips, and tongue, corneal lacerations, palmar hyperkeratosis, non-painful fracture, and joint deformities in the right ankle. Tearing, deep tendon reflexes, and motor and sensory nerve action potentials were normal [10].
Case Study 3: A case report of CIPA [10]
A 2.5-year-old boy was referred to the paediatrics clinic with severe self-mutilating injuries to his hands, feet, tongue, and oral mucosa caused by unconscious biting. He is the second child of parents who were cousins. He was born full term through normal vaginal delivery with a birth weight of 3300 gr. At two-months of age, he was admitted to the hospital for fever and convulsion. The patient continued to have fever during his hospital admission, where evaluation for the aetiology of prolonged fever was done and abnormal results were not seen in any of the diagnostic tests. His parents reported that he never experienced sweating after birth, could not tolerate warm weather or sun exposure, and became irritable and teary in these situations. The parents also noted that he showed no response to any kind of injury including pinpricking, burning, hitting, and cutting. When 2.5 years old, he received outpatient services for a right third metatarsal fracture of an unclear nature which caused oedema and deformity in his right foot. Teething had started at seven months of age, but because of biting and ulcerative lesions in the gums, his teeth had started to shed at 1.5 years of age. Ulcerative lesions were seen in his fingers, toes, and mouth that were also caused by self-biting [10].
In addition, keratosis and thick, dry skin were visible on the palms of his hands and soles of his feet. He also had red eyes and a corneal ulcer. Charcot joint (neuropathic osteoarthropathy) was observed in his right ankle due to repeated trauma. On the other hand, neurologic examination revealed normal function of the cranial nerves. The light response of his pupils and deep tendon reflexes (DTR) were normal. His plantar reflex was flexor bilaterally, however, he could not cooperate with the sensory exam. The patient also completed the Denver Developmental Screening Test-II which indicated a neurodevelopmental delay [10].

Figure 2. Examples of common CIPA clinical presentations [11]
Diagnosis
Diagnosis of CIPA involves a combination of clinical evaluation and specialised tests. Nerve conduction studies (NCS) and electromyography (EMG) are commonly used to assess the function of peripheral nerves and muscles in individuals suspected of having CIPA [12]. In CIPA patients, NCS may reveal absence or significant reduction in sensory nerve action potentials (SNAPs), indicating impaired sensory nerve function, while EMG typically shows normal findings as motor nerves are usually unaffected in CIPA. Genetic testing to identify mutations in the NTRK1 gene is also crucial for confirming a diagnosis of CIPA [12].
Management
CIPA care typically focuses on symptom management and prevention of complications. There is currently no cure for CIPA, thus treatment is aimed at addressing specific symptoms and minimisation of risks [13]. Early recognition of CIPA, along with prenatal screening for at-risk couples, can help prevent the birth of affected children. Specific management strategies, such as regular follow up for visual/optical and dental care can reduce the frequency and severity of complications in individuals with CIPA [13].
Conclusion
In the realm of neurological disorders, CIPA stands as a poignant paradox, where the absence of pain brings forth profound suffering. Delving into this rare condition, it becomes evident that its impact extends far beyond the individual, affecting families and communities. Through the examination of case studies and clinical insights, the complex interplay of physiological abnormalities and clinical manifestations emerges, painting a vivid picture of the challenges faced by those living with CIPA. Despite its rarity, the need for heightened awareness within the medical community is undeniable, urging for a concerted effort in early detection and tailored management strategies. As we navigate the intricacies of CIPA, it becomes apparent that behind the veil of painlessness lies a profound journey of resilience and adaptation. In shedding light on this overlooked disorder, we pave the way for greater understanding, compassion, and support for those impacted by the pain of painlessness.
References
Indo Y. Genetics of congenital insensitivity to pain with anhidrosis (CIPA) or hereditary sensory and autonomic neuropathy type IV. Clinical Autonomic Research. 2002;12(Suppl 1):I2-5. [DOI: 10.1007/s10286-002-0029-x]
Indo Y. Neurobiology of pain, interoception, and emotional response: lessons from nerve growth factor-dependent neurons. European Journal of Neuroscience. 2014;39(3):375-391. [DOI: 10.1111/ejn.12444]
Indo, Y. (2017) Figure 1, Science Direct. Neuroscience & Biobehavioral Review. Available at: https://www.sciencedirect.com/science/article/pii/S0149763417307121#fig0005 (Accessed: 09 May 2024).
Rosemberg S, Marie SK, Kliemann S. Congenital insensitivity to pain with anhidrosis (hereditary sensory and autonomic neuropathy type IV). Pediatric Neurology. 1994;11(1):50-56. [DOI: 10.1016/0887-8994(94)90012-4]
Thakur S, Ganguly A, Anand KS, et al. Clinical and molecular genetic analysis of 19 families with hereditary sensory and autonomic neuropathy type IV - Report of 11 novel mutations. European Journal of Medical Genetics. 2018;61(8):433-441. [DOI: 10.1016/j.ejmg.2018.02.008]
Linton S. Understanding Pain for Better Clinical Practice: A Psychological Perspective. Elsevier Health Sciences. 2005. ISBN 978-0444515919.
Drenth JP, Waxman SG. Mutations in sodium-channel gene SCN9A cause a spectrum of human genetic pain disorders. The Journal of Clinical Investigation. 2007;117(12):3603-3609. [DOI: 10.1172/JCI33297]
Liu Z, Liu J, Liu G, et al. Phenotypic heterogeneity of intellectual disability in patients with congenital insensitivity to pain with anhidrosis: A case report and literature review. Journal of International Medical Research. 2018;46(6):2445-2457. [DOI: 10.1177/0300060517747164]
Zhang M, Cao X, Li N, et al. Autism spectrum disorder in a boy with congenital insensitivity to pain with anhidrosis: a case report. BMC Pediatrics. 2022;22:126. [DOI: 10.1186/s12887-022-03196-3]
Karimi M, Fa Llah R. A Case Report of Congenital Insensitivity to Pain and Anhidrosis (CIPA). Iran J Child Neurol. 2012 Summer;6(3):45-8. PMID: 24665272; PMCID: PMC3943025.
Li, N. et al. (2019) Pictures depicting common clinical features of patients, Research Gate. Dovepress. Available at: https://www.researchgate.net/publication/330527642_Heterogeneity_of_clinical_features_and_mutation_analysis_of_NTRK1_in_Han_Chinese_patients_with_congenital_insensitivity_to_pain_with_anhidrosis (Accessed: 09 May 2024).
Shatzky S, Moses S, Levy J, et al. Congenital insensitivity to pain with anhidrosis (CIPA) in Israeli-Bedouins: genetic heterogeneity, novel mutations in the TRKA/NGF receptor gene, clinical findings, and results of nerve conduction studies. American Journal of Medical Genetics. 2000;92(5):353-360. [DOI: 10.1002/1096-8628(20000731)92:5<353::aid-ajmg9>3.0.co;2-n]
Einarsdottir E, Carlsson A, Minde J, et al. A mutation in the nerve growth factor beta gene (NGFB) causes loss of pain perception. Human Molecular Genetics. 2004;13(8):799-805. [DOI: 10.1093/hmg/ddh096]